
Image above: A masked worker cleans a New York City subway entrance.
How did it come to this? A virus a thousand times smaller than a dust mote has humbled and humiliated the planet’s most powerful nation. America has failed to protect its people, leaving them with illness and financial ruin. It has lost its status as a global leader. It has careened between inaction and ineptitude. The breadth and magnitude of its errors are difficult, in the moment, to truly fathom.
To hear more feature stories, get the Audm iPhone app.
In the first half of 2020, SARS‑CoV‑2—the new coronavirus behind the disease COVID‑19—infected 10 million people around the world and killed about half a million. But few countries have been as severely hit as the United States, which has just 4 percent of the world’s population but a quarter of its confirmed COVID‑19 cases and deaths. These numbers are estimates. The actual toll, though undoubtedly higher, is unknown, because the richest country in the world still lacks sufficient testing to accurately count its sick citizens.
Despite ample warning, the U.S. squandered every possible opportunity to control the coronavirus. And despite its considerable advantages—immense resources, biomedical might, scientific expertise—it floundered. While countries as different as South Korea, Thailand, Iceland, Slovakia, and Australia acted decisively to bend the curve of infections downward, the U.S. achieved merely a plateau in the spring, which changed to an appalling upward slope in the summer. “The U.S. fundamentally failed in ways that were worse than I ever could have imagined,” Julia Marcus, an infectious-disease epidemiologist at Harvard Medical School, told me.
Since the pandemic began, I have spoken with more than 100 experts in a variety of fields. I’ve learned that almost everything that went wrong with America’s response to the pandemic was predictable and preventable. A sluggish response by a government denuded of expertise allowed the coronavirus to gain a foothold. Chronic underfunding of public health neutered the nation’s ability to prevent the pathogen’s spread. A bloated, inefficient health-care system left hospitals ill-prepared for the ensuing wave of sickness. Racist policies that have endured since the days of colonization and slavery left Indigenous and Black Americans especially vulnerable to COVID‑19. The decades-long process of shredding the nation’s social safety net forced millions of essential workers in low-paying jobs to risk their life for their livelihood. The same social-media platforms that sowed partisanship and misinformation during the 2014 Ebola outbreak in Africa and the 2016 U.S. election became vectors for conspiracy theories during the 2020 pandemic.
The U.S. has little excuse for its inattention. In recent decades, epidemics of SARS, MERS, Ebola, H1N1 flu, Zika, and monkeypox showed the havoc that new and reemergent pathogens could wreak. Health experts, business leaders, and even middle schoolers ran simulated exercises to game out the spread of new diseases. In 2018, I wrote an article for The Atlantic arguing that the U.S. was not ready for a pandemic, and sounded warnings about the fragility of the nation’s health-care system and the slow process of creating a vaccine. But the COVID‑19 debacle has also touched—and implicated—nearly every other facet of American society: its shortsighted leadership, its disregard for expertise, its racial inequities, its social-media culture, and its fealty to a dangerous strain of individualism.
SARS‑CoV‑2 is something of an anti-Goldilocks virus: just bad enough in every way. Its symptoms can be severe enough to kill millions but are often mild enough to allow infections to move undetected through a population. It spreads quickly enough to overload hospitals, but slowly enough that statistics don’t spike until too late. These traits made the virus harder to control, but they also softened the pandemic’s punch. SARS‑CoV‑2 is neither as lethal as some other coronaviruses, such as SARS and MERS, nor as contagious as measles. Deadlier pathogens almost certainly exist. Wild animals harbor an estimated 40,000 unknown viruses, a quarter of which could potentially jump into humans. How will the U.S. fare when “we can’t even deal with a starter pandemic?,” Zeynep Tufekci, a sociologist at the University of North Carolina and an Atlantic contributing writer, asked me.
Despite its epochal effects, COVID‑19 is merely a harbinger of worse plagues to come. The U.S. cannot prepare for these inevitable crises if it returns to normal, as many of its people ache to do. Normal led to this. Normal was a world ever more prone to a pandemic but ever less ready for one. To avert another catastrophe, the U.S. needs to grapple with all the ways normal failed us. It needs a full accounting of every recent misstep and foundational sin, every unattended weakness and unheeded warning, every festering wound and reopened scar.
A pandemic can be prevented in two ways: Stop an infection from ever arising, or stop an infection from becoming thousands more. The first way is likely impossible. There are simply too many viruses and too many animals that harbor them. Bats alone could host thousands of unknown coronaviruses; in some Chinese caves, one out of every 20 bats is infected. Many people live near these caves, shelter in them, or collect guano from them for fertilizer. Thousands of bats also fly over these people’s villages and roost in their homes, creating opportunities for the bats’ viral stowaways to spill over into human hosts. Based on antibody testing in rural parts of China, Peter Daszak of EcoHealth Alliance, a nonprofit that studies emerging diseases, estimates that such viruses infect a substantial number of people every year. “Most infected people don’t know about it, and most of the viruses aren’t transmissible,” Daszak says. But it takes just one transmissible virus to start a pandemic.
Sometime in late 2019, the wrong virus left a bat and ended up, perhaps via an intermediate host, in a human—and another, and another. Eventually it found its way to the Huanan seafood market, and jumped into dozens of new hosts in an explosive super-spreading event. The COVID‑19 pandemic had begun.
“There is no way to get spillover of everything to zero,” Colin Carlson, an ecologist at Georgetown University, told me. Many conservationists jump on epidemics as opportunities to ban the wildlife trade or the eating of “bush meat,” an exoticized term for “game,” but few diseases have emerged through either route. Carlson said the biggest factors behind spillovers are land-use change and climate change, both of which are hard to control. Our species has relentlessly expanded into previously wild spaces. Through intensive agriculture, habitat destruction, and rising temperatures, we have uprooted the planet’s animals, forcing them into new and narrower ranges that are on our own doorsteps. Humanity has squeezed the world’s wildlife in a crushing grip—and viruses have come bursting out.
Curtailing those viruses after they spill over is more feasible, but requires knowledge, transparency, and decisiveness that were lacking in 2020. Much about coronaviruses is still unknown. There are no surveillance networks for detecting them as there are for influenza. There are no approved treatments or vaccines. Coronaviruses were formerly a niche family, of mainly veterinary importance. Four decades ago, just 60 or so scientists attended the first international meeting on coronaviruses. Their ranks swelled after SARS swept the world in 2003, but quickly dwindled as a spike in funding vanished. The same thing happened after MERS emerged in 2012. This year, the world’s coronavirus experts—and there still aren’t many—had to postpone their triennial conference in the Netherlands because SARS‑CoV‑2 made flying too risky.
In the age of cheap air travel, an outbreak that begins on one continent can easily reach the others. SARS already demonstrated that in 2003, and more than twice as many people now travel by plane every year. To avert a pandemic, affected nations must alert their neighbors quickly. In 2003, China covered up the early spread of SARS, allowing the new disease to gain a foothold, and in 2020, history repeated itself. The Chinese government downplayed the possibility that SARS‑CoV‑2 was spreading among humans, and only confirmed as much on January 20, after millions had traveled around the country for the lunar new year. Doctors who tried to raise the alarm were censured and threatened. One, Li Wenliang, later died of COVID‑19. The World Health Organization initially parroted China’s line and did not declare a public-health emergency of international concern until January 30. By then, an estimated 10,000 people in 20 countries had been infected, and the virus was spreading fast.
The United States has correctly castigated China for its duplicity and the WHO for its laxity—but the U.S. has also failed the international community. Under President Donald Trump, the U.S. has withdrawn from several international partnerships and antagonized its allies. It has a seat on the WHO’s executive board, but left that position empty for more than two years, only filling it this May, when the pandemic was in full swing. Since 2017, Trump has pulled more than 30 staffers out of the Centers for Disease Control and Prevention’s office in China, who could have warned about the spreading coronavirus. Last July, he defunded an American epidemiologist embedded within China’s CDC. America First was America oblivious.
Even after warnings reached the U.S., they fell on the wrong ears. Since before his election, Trump has cavalierly dismissed expertise and evidence. He filled his administration with inexperienced newcomers, while depicting career civil servants as part of a “deep state.” In 2018, he dismantled an office that had been assembled specifically to prepare for nascent pandemics. American intelligence agencies warned about the coronavirus threat in January, but Trump habitually disregards intelligence briefings. The secretary of health and human services, Alex Azar, offered similar counsel, and was twice ignored.
Being prepared means being ready to spring into action, “so that when something like this happens, you’re moving quickly,” Ronald Klain, who coordinated the U.S. response to the West African Ebola outbreak in 2014, told me. “By early February, we should have triggered a series of actions, precisely zero of which were taken.” Trump could have spent those crucial early weeks mass-producing tests to detect the virus, asking companies to manufacture protective equipment and ventilators, and otherwise steeling the nation for the worst. Instead, he focused on the border. On January 31, Trump announced that the U.S. would bar entry to foreigners who had recently been in China, and urged Americans to avoid going there.
Travel bans make intuitive sense, because travel obviously enables the spread of a virus. But in practice, travel bans are woefully inefficient at restricting either travel or viruses. They prompt people to seek indirect routes via third-party countries, or to deliberately hide their symptoms. They are often porous: Trump’s included numerous exceptions, and allowed tens of thousands of people to enter from China. Ironically, they create travel: When Trump later announced a ban on flights from continental Europe, a surge of travelers packed America’s airports in a rush to beat the incoming restrictions. Travel bans may sometimes work for remote island nations, but in general they can only delay the spread of an epidemic—not stop it. And they can create a harmful false confidence, so countries “rely on bans to the exclusion of the things they actually need to do—testing, tracing, building up the health system,” says Thomas Bollyky, a global-health expert at the Council on Foreign Relations. “That sounds an awful lot like what happened in the U.S.”
This was predictable. A president who is fixated on an ineffectual border wall, and has portrayed asylum seekers as vectors of disease, was always going to reach for travel bans as a first resort. And Americans who bought into his rhetoric of xenophobia and isolationism were going to be especially susceptible to thinking that simple entry controls were a panacea.
And so the U.S. wasted its best chance of restraining COVID‑19. Although the disease first arrived in the U.S. in mid-January, genetic evidence shows that the specific viruses that triggered the first big outbreaks, in Washington State, didn’t land until mid-February. The country could have used that time to prepare. Instead, Trump, who had spent his entire presidency learning that he could say whatever he wanted without consequence, assured Americans that “the coronavirus is very much under control,” and “like a miracle, it will disappear.” With impunity, Trump lied. With impunity, the virus spread.
On February 26, Trump asserted that cases were “going to be down to close to zero.” Over the next two months, at least 1 million Americans were infected.

As the coronavirus established itself in the U.S., it found a nation through which it could spread easily, without being detected. For years, Pardis Sabeti, a virologist at the Broad Institute of Harvard and MIT, has been trying to create a surveillance network that would allow hospitals in every major U.S. city to quickly track new viruses through genetic sequencing. Had that network existed, once Chinese scientists published SARS‑CoV‑2’s genome on January 11, every American hospital would have been able to develop its own diagnostic test in preparation for the virus’s arrival. “I spent a lot of time trying to convince many funders to fund it,” Sabeti told me. “I never got anywhere.”
The CDC developed and distributed its own diagnostic tests in late January. These proved useless because of a faulty chemical component. Tests were in such short supply, and the criteria for getting them were so laughably stringent, that by the end of February, tens of thousands of Americans had likely been infected but only hundreds had been tested. The official data were so clearly wrong that The Atlantic developed its own volunteer-led initiative—the COVID Tracking Project—to count cases.
Diagnostic tests are easy to make, so the U.S. failing to create one seemed inconceivable. Worse, it had no Plan B. Private labs were strangled by FDA bureaucracy. Meanwhile, Sabeti’s lab developed a diagnostic test in mid-January and sent it to colleagues in Nigeria, Sierra Leone, and Senegal. “We had working diagnostics in those countries well before we did in any U.S. states,” she told me.
It’s hard to overstate how thoroughly the testing debacle incapacitated the U.S. People with debilitating symptoms couldn’t find out what was wrong with them. Health officials couldn’t cut off chains of transmission by identifying people who were sick and asking them to isolate themselves.
[Read: How the coronavirus became an American catastrophe]
Water running along a pavement will readily seep into every crack; so, too, did the unchecked coronavirus seep into every fault line in the modern world. Consider our buildings. In response to the global energy crisis of the 1970s, architects made structures more energy-efficient by sealing them off from outdoor air, reducing ventilation rates. Pollutants and pathogens built up indoors, “ushering in the era of ‘sick buildings,’ ” says Joseph Allen, who studies environmental health at Harvard’s T. H. Chan School of Public Health. Energy efficiency is a pillar of modern climate policy, but there are ways to achieve it without sacrificing well-being. “We lost our way over the years and stopped designing buildings for people,” Allen says.
The indoor spaces in which Americans spend 87 percent of their time became staging grounds for super-spreading events. One study showed that the odds of catching the virus from an infected person are roughly 19 times higher indoors than in open air. Shielded from the elements and among crowds clustered in prolonged proximity, the coronavirus ran rampant in the conference rooms of a Boston hotel, the cabins of the Diamond Princess cruise ship, and a church hall in Washington State where a choir practiced for just a few hours.
The hardest-hit buildings were those that had been jammed with people for decades: prisons. Between harsher punishments doled out in the War on Drugs and a tough-on-crime mindset that prizes retribution over rehabilitation, America’s incarcerated population has swelled sevenfold since the 1970s, to about 2.3 million. The U.S. imprisons five to 18 times more people per capita than other Western democracies. Many American prisons are packed beyond capacity, making social distancing impossible. Soap is often scarce. Inevitably, the coronavirus ran amok. By June, two American prisons each accounted for more cases than all of New Zealand. One, Marion Correctional Institution, in Ohio, had more than 2,000 cases among inmates despite having a capacity of 1,500.

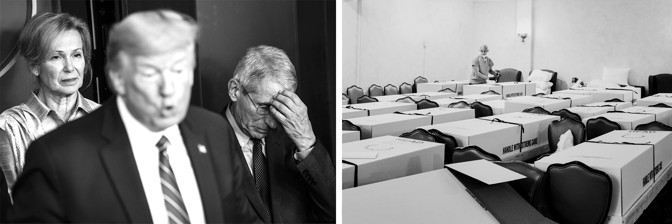
Other densely packed facilities were also besieged. America’s nursing homes and long-term-care facilities house less than 1 percent of its people, but as of mid-June, they accounted for 40 percent of its coronavirus deaths. More than 50,000 residents and staff have died. At least 250,000 more have been infected. These grim figures are a reflection not just of the greater harms that COVID‑19 inflicts upon elderly physiology, but also of the care the elderly receive. Before the pandemic, three in four nursing homes were understaffed, and four in five had recently been cited for failures in infection control. The Trump administration’s policies have exacerbated the problem by reducing the influx of immigrants, who make up a quarter of long-term caregivers.
[Read: Another coronavirus nursing-home disaster is coming]
Even though a Seattle nursing home was one of the first COVID‑19 hot spots in the U.S., similar facilities weren’t provided with tests and protective equipment. Rather than girding these facilities against the pandemic, the Department of Health and Human Services paused nursing-home inspections in March, passing the buck to the states. Some nursing homes avoided the virus because their owners immediately stopped visitations, or paid caregivers to live on-site. But in others, staff stopped working, scared about infecting their charges or becoming infected themselves. In some cases, residents had to be evacuated because no one showed up to care for them.
America’s neglect of nursing homes and prisons, its sick buildings, and its botched deployment of tests are all indicative of its problematic attitude toward health: “Get hospitals ready and wait for sick people to show,” as Sheila Davis, the CEO of the nonprofit Partners in Health, puts it. “Especially in the beginning, we catered our entire [COVID‑19] response to the 20 percent of people who required hospitalization, rather than preventing transmission in the community.” The latter is the job of the public-health system, which prevents sickness in populations instead of merely treating it in individuals. That system pairs uneasily with a national temperament that views health as a matter of personal responsibility rather than a collective good.
At the end of the 20th century, public-health improvements meant that Americans were living an average of 30 years longer than they were at the start of it. Maternal mortality had fallen by 99 percent; infant mortality by 90 percent. Fortified foods all but eliminated rickets and goiters. Vaccines eradicated smallpox and polio, and brought measles, diphtheria, and rubella to heel. These measures, coupled with antibiotics and better sanitation, curbed infectious diseases to such a degree that some scientists predicted they would soon pass into history. But instead, these achievements brought complacency. “As public health did its job, it became a target” of budget cuts, says Lori Freeman, the CEO of the National Association of County and City Health Officials.
Today, the U.S. spends just 2.5 percent of its gigantic health-care budget on public health. Underfunded health departments were already struggling to deal with opioid addiction, climbing obesity rates, contaminated water, and easily preventable diseases. Last year saw the most measles cases since 1992. In 2018, the U.S. had 115,000 cases of syphilis and 580,000 cases of gonorrhea—numbers not seen in almost three decades. It has 1.7 million cases of chlamydia, the highest number ever recorded.
Since the last recession, in 2009, chronically strapped local health departments have lost 55,000 jobs—a quarter of their workforce. When COVID‑19 arrived, the economic downturn forced overstretched departments to furlough more employees. When states needed battalions of public-health workers to find infected people and trace their contacts, they had to hire and train people from scratch. In May, Maryland Governor Larry Hogan asserted that his state would soon have enough people to trace 10,000 contacts every day. Last year, as Ebola tore through the Democratic Republic of Congo—a country with a quarter of Maryland’s wealth and an active war zone—local health workers and the WHO traced twice as many people.

Ripping unimpeded through American communities, the coronavirus created thousands of sickly hosts that it then rode into America’s hospitals. It should have found facilities armed with state-of-the-art medical technologies, detailed pandemic plans, and ample supplies of protective equipment and life-saving medicines. Instead, it found a brittle system in danger of collapse.
Compared with the average wealthy nation, America spends nearly twice as much of its national wealth on health care, about a quarter of which is wasted on inefficient care, unnecessary treatments, and administrative chicanery. The U.S. gets little bang for its exorbitant buck. It has the lowest life-expectancy rate of comparable countries, the highest rates of chronic disease, and the fewest doctors per person. This profit-driven system has scant incentive to invest in spare beds, stockpiled supplies, peacetime drills, and layered contingency plans—the essence of pandemic preparedness. America’s hospitals have been pruned and stretched by market forces to run close to full capacity, with little ability to adapt in a crisis.
When hospitals do create pandemic plans, they tend to fight the last war. After 2014, several centers created specialized treatment units designed for Ebola—a highly lethal but not very contagious disease. These units were all but useless against a highly transmissible airborne virus like SARS‑CoV‑2. Nor were hospitals ready for an outbreak to drag on for months. Emergency plans assumed that staff could endure a few days of exhausting conditions, that supplies would hold, and that hard-hit centers could be supported by unaffected neighbors. “We’re designed for discrete disasters” like mass shootings, traffic pileups, and hurricanes, says Esther Choo, an emergency physician at Oregon Health and Science University. The COVID‑19 pandemic is not a discrete disaster. It is a 50-state catastrophe that will likely continue at least until a vaccine is ready.
Wherever the coronavirus arrived, hospitals reeled. Several states asked medical students to graduate early, reenlisted retired doctors, and deployed dermatologists to emergency departments. Doctors and nurses endured grueling shifts, their faces chapped and bloody when they finally doffed their protective equipment. Soon, that equipment—masks, respirators, gowns, gloves—started running out.
American hospitals operate on a just-in-time economy. They acquire the goods they need in the moment through labyrinthine supply chains that wrap around the world in tangled lines, from countries with cheap labor to richer nations like the U.S. The lines are invisible until they snap. About half of the world’s face masks, for example, are made in China, some of them in Hubei province. When that region became the pandemic epicenter, the mask supply shriveled just as global demand spiked. The Trump administration turned to a larder of medical supplies called the Strategic National Stockpile, only to find that the 100 million respirators and masks that had been dispersed during the 2009 flu pandemic were never replaced. Just 13 million respirators were left.
In April, four in five frontline nurses said they didn’t have enough protective equipment. Some solicited donations from the public, or navigated a morass of back-alley deals and internet scams. Others fashioned their own surgical masks from bandannas and gowns from garbage bags. The supply of nasopharyngeal swabs that are used in every diagnostic test also ran low, because one of the largest manufacturers is based in Lombardy, Italy—initially the COVID‑19 capital of Europe. About 40 percent of critical-care drugs, including antibiotics and painkillers, became scarce because they depend on manufacturing lines that begin in China and India. Once a vaccine is ready, there might not be enough vials to put it in, because of the long-running global shortage of medical-grade glass—literally, a bottle-neck bottleneck.
The federal government could have mitigated those problems by buying supplies at economies of scale and distributing them according to need. Instead, in March, Trump told America’s governors to “try getting it yourselves.” As usual, health care was a matter of capitalism and connections. In New York, rich hospitals bought their way out of their protective-equipment shortfall, while neighbors in poorer, more diverse parts of the city rationed their supplies.
While the president prevaricated, Americans acted. Businesses sent their employees home. People practiced social distancing, even before Trump finally declared a national emergency on March 13, and before governors and mayors subsequently issued formal stay-at-home orders, or closed schools, shops, and restaurants. A study showed that the U.S. could have averted 36,000 COVID‑19 deaths if leaders had enacted social-distancing measures just a week earlier. But better late than never: By collectively reducing the spread of the virus, America flattened the curve. Ventilators didn’t run out, as they had in parts of Italy. Hospitals had time to add extra beds.
Social distancing worked. But the indiscriminate lockdown was necessary only because America’s leaders wasted months of prep time. Deploying this blunt policy instrument came at enormous cost. Unemployment rose to 14.7 percent, the highest level since record-keeping began, in 1948. More than 26 million people lost their jobs, a catastrophe in a country that—uniquely and absurdly—ties health care to employment. Some COVID‑19 survivors have been hit with seven-figure medical bills. In the middle of the greatest health and economic crises in generations, millions of Americans have found themselves disconnected from medical care and impoverished. They join the millions who have always lived that way.

The coronavirus found, exploited, and widened every inequity that the U.S. had to offer. Elderly people, already pushed to the fringes of society, were treated as acceptable losses. Women were more likely to lose jobs than men, and also shouldered extra burdens of child care and domestic work, while facing rising rates of domestic violence. In half of the states, people with dementia and intellectual disabilities faced policies that threatened to deny them access to lifesaving ventilators. Thousands of people endured months of COVID‑19 symptoms that resembled those of chronic postviral illnesses, only to be told that their devastating symptoms were in their head. Latinos were three times as likely to be infected as white people. Asian Americans faced racist abuse. Far from being a “great equalizer,” the pandemic fell unevenly upon the U.S., taking advantage of injustices that had been brewing throughout the nation’s history.
[Read: COVID-19 can last for several months]
Of the 3.1 million Americans who cannot afford health insurance, more than half are people of color, and 30 percent are Black. This is no accident. In the decades after the Civil War, the white leaders of former slave states deliberately withheld health care from Black Americans, apportioning medicine more according to the logic of Jim Crow than Hippocrates. They built hospitals away from Black communities, segregated Black patients into separate wings, and blocked Black students from medical school. In the 20th century, they helped construct America’s system of private, employer-based insurance, which has kept many Black people from receiving adequate medical treatment. They fought every attempt to improve Black people’s access to health care, from the creation of Medicare and Medicaid in the ’60s to the passage of the Affordable Care Act in 2010.
A number of former slave states also have among the lowest investments in public health, the lowest quality of medical care, the highest proportions of Black citizens, and the greatest racial divides in health outcomes. As the COVID‑19 pandemic wore on, they were among the quickest to lift social-distancing restrictions and reexpose their citizens to the coronavirus. The harms of these moves were unduly foisted upon the poor and the Black.
As of early July, one in every 1,450 Black Americans had died from COVID‑19—a rate more than twice that of white Americans. That figure is both tragic and wholly expected given the mountain of medical disadvantages that Black people face. Compared with white people, they die three years younger. Three times as many Black mothers die during pregnancy. Black people have higher rates of chronic illnesses that predispose them to fatal cases of COVID‑19. When they go to hospitals, they’re less likely to be treated. The care they do receive tends to be poorer. Aware of these biases, Black people are hesitant to seek aid for COVID‑19 symptoms and then show up at hospitals in sicker states. “One of my patients said, ‘I don’t want to go to the hospital, because they’re not going to treat me well,’ ” says Uché Blackstock, an emergency physician and the founder of Advancing Health Equity, a nonprofit that fights bias and racism in health care. “Another whispered to me, ‘I’m so relieved you’re Black. I just want to make sure I’m listened to.’ ”
Black people were both more worried about the pandemic and more likely to be infected by it. The dismantling of America’s social safety net left Black people with less income and higher unemployment. They make up a disproportionate share of the low-paid “essential workers” who were expected to staff grocery stores and warehouses, clean buildings, and deliver mail while the pandemic raged around them. Earning hourly wages without paid sick leave, they couldn’t afford to miss shifts even when symptomatic. They faced risky commutes on crowded public transportation while more privileged people teleworked from the safety of isolation. “There’s nothing about Blackness that makes you more prone to COVID,” says Nicolette Louissaint, the executive director of Healthcare Ready, a nonprofit that works to strengthen medical supply chains. Instead, existing inequities stack the odds in favor of the virus.
Native Americans were similarly vulnerable. A third of the people in the Navajo Nation can’t easily wash their hands, because they’ve been embroiled in long-running negotiations over the rights to the water on their own lands. Those with water must contend with runoff from uranium mines. Most live in cramped multigenerational homes, far from the few hospitals that service a 17-million-acre reservation. As of mid-May, the Navajo Nation had higher rates of COVID‑19 infections than any U.S. state.
Americans often misperceive historical inequities as personal failures. Stephen Huffman, a Republican state senator and doctor in Ohio, suggested that Black Americans might be more prone to COVID‑19 because they don’t wash their hands enough, a remark for which he later apologized. Republican Senator Bill Cassidy of Louisiana, also a physician, noted that Black people have higher rates of chronic disease, as if this were an answer in itself, and not a pattern that demanded further explanation.
Clear distribution of accurate information is among the most important defenses against an epidemic’s spread. And yet the largely unregulated, social-media-based communications infrastructure of the 21st century almost ensures that misinformation will proliferate fast. “In every outbreak throughout the existence of social media, from Zika to Ebola, conspiratorial communities immediately spread their content about how it’s all caused by some government or pharmaceutical company or Bill Gates,” says Renée DiResta of the Stanford Internet Observatory, who studies the flow of online information. When COVID‑19 arrived, “there was no doubt in my mind that it was coming.”
[Read: The great 5G conspiracy]
Sure enough, existing conspiracy theories—George Soros! 5G! Bioweapons!—were repurposed for the pandemic. An infodemic of falsehoods spread alongside the actual virus. Rumors coursed through online platforms that are designed to keep users engaged, even if that means feeding them content that is polarizing or untrue. In a national crisis, when people need to act in concert, this is calamitous. “The social internet as a system is broken,” DiResta told me, and its faults are readily abused.

Beginning on April 16, DiResta’s team noticed growing online chatter about Judy Mikovits, a discredited researcher turned anti-vaccination champion. Posts and videos cast Mikovits as a whistleblower who claimed that the new coronavirus was made in a lab and described Anthony Fauci of the White House’s coronavirus task force as her nemesis. Ironically, this conspiracy theory was nested inside a larger conspiracy—part of an orchestrated PR campaign by an anti-vaxxer and QAnon fan with the explicit goal to “take down Anthony Fauci.” It culminated in a slickly produced video called Plandemic, which was released on May 4. More than 8 million people watched it in a week.
Doctors and journalists tried to debunk Plandemic’s many misleading claims, but these efforts spread less successfully than the video itself. Like pandemics, infodemics quickly become uncontrollable unless caught early. But while health organizations recognize the need to surveil for emerging diseases, they are woefully unprepared to do the same for emerging conspiracies. In 2016, when DiResta spoke with a CDC team about the threat of misinformation, “their response was: ‘ That’s interesting, but that’s just stuff that happens on the internet.’ ”
[From the June 2020 issue: Adrienne LaFrance on how QAnon is more important than you think]
Rather than countering misinformation during the pandemic’s early stages, trusted sources often made things worse. Many health experts and government officials downplayed the threat of the virus in January and February, assuring the public that it posed a low risk to the U.S. and drawing comparisons to the ostensibly greater threat of the flu. The WHO, the CDC, and the U.S. surgeon general urged people not to wear masks, hoping to preserve the limited stocks for health-care workers. These messages were offered without nuance or acknowledgement of uncertainty, so when they were reversed—the virus is worse than the flu; wear masks—the changes seemed like befuddling flip-flops.
The media added to the confusion. Drawn to novelty, journalists gave oxygen to fringe anti-lockdown protests while most Americans quietly stayed home. They wrote up every incremental scientific claim, even those that hadn’t been verified or peer-reviewed.
There were many such claims to choose from. By tying career advancement to the publishing of papers, academia already creates incentives for scientists to do attention-grabbing but irreproducible work. The pandemic strengthened those incentives by prompting a rush of panicked research and promising ambitious scientists global attention.

In March, a small and severely flawed French study suggested that the antimalarial drug hydroxychloroquine could treat COVID‑19. Published in a minor journal, it likely would have been ignored a decade ago. But in 2020, it wended its way to Donald Trump via a chain of credulity that included Fox News, Elon Musk, and Dr. Oz. Trump spent months touting the drug as a miracle cure despite mounting evidence to the contrary, causing shortages for people who actually needed it to treat lupus and rheumatoid arthritis. The hydroxychloroquine story was muddied even further by two studies published in top medical journals—The Lancet and the New England Journal of Medicine—that claimed the drug was not effective and was potentially harmful. The papers relied on suspect data from a small analytics company called Surgisphere. Both were retracted in June.
Science famously self-corrects. But during the pandemic, the same urgent pace that has produced valuable knowledge at record speed has also sent sloppy claims around the world before anyone could even raise a skeptical eyebrow. The ensuing confusion, and the many genuine unknowns about the virus, has created a vortex of fear and uncertainty, which grifters have sought to exploit. Snake-oil merchants have peddled ineffectual silver bullets (including actual silver). Armchair experts with scant or absent qualifications have found regular slots on the nightly news. And at the center of that confusion is Donald Trump.
During a pandemic, leaders must rally the public, tell the truth, and speak clearly and consistently. Instead, Trump repeatedly contradicted public-health experts, his scientific advisers, and himself. He said that “nobody ever thought a thing like [the pandemic] could happen” and also that he “felt it was a pandemic long before it was called a pandemic.” Both statements cannot be true at the same time, and in fact neither is true.
A month before his inauguration, I wrote that “the question isn’t whether [Trump will] face a deadly outbreak during his presidency, but when.” Based on his actions as a media personality during the 2014 Ebola outbreak and as a candidate in the 2016 election, I suggested that he would fail at diplomacy, close borders, tweet rashly, spread conspiracy theories, ignore experts, and exhibit reckless self-confidence. And so he did.
No one should be shocked that a liar who has made almost 20,000 false or misleading claims during his presidency would lie about whether the U.S. had the pandemic under control; that a racist who gave birth to birtherism would do little to stop a virus that was disproportionately killing Black people; that a xenophobe who presided over the creation of new immigrant-detention centers would order meatpacking plants with a substantial immigrant workforce to remain open; that a cruel man devoid of empathy would fail to calm fearful citizens; that a narcissist who cannot stand to be upstaged would refuse to tap the deep well of experts at his disposal; that a scion of nepotism would hand control of a shadow coronavirus task force to his unqualified son-in-law; that an armchair polymath would claim to have a “natural ability” at medicine and display it by wondering out loud about the curative potential of injecting disinfectant; that an egotist incapable of admitting failure would try to distract from his greatest one by blaming China, defunding the WHO, and promoting miracle drugs; or that a president who has been shielded by his party from any shred of accountability would say, when asked about the lack of testing, “I don’t take any responsibility at all.”

Trump is a comorbidity of the COVID‑19 pandemic. He isn’t solely responsible for America’s fiasco, but he is central to it. A pandemic demands the coordinated efforts of dozens of agencies. “In the best circumstances, it’s hard to make the bureaucracy move quickly,” Ron Klain said. “It moves if the president stands on a table and says, ‘Move quickly.’ But it really doesn’t move if he’s sitting at his desk saying it’s not a big deal.”
In the early days of Trump’s presidency, many believed that America’s institutions would check his excesses. They have, in part, but Trump has also corrupted them. The CDC is but his latest victim. On February 25, the agency’s respiratory-disease chief, Nancy Messonnier, shocked people by raising the possibility of school closures and saying that “disruption to everyday life might be severe.” Trump was reportedly enraged. In response, he seems to have benched the entire agency. The CDC led the way in every recent domestic disease outbreak and has been the inspiration and template for public-health agencies around the world. But during the three months when some 2 million Americans contracted COVID‑19 and the death toll topped 100,000, the agency didn’t hold a single press conference. Its detailed guidelines on reopening the country were shelved for a month while the White House released its own uselessly vague plan.
Again, everyday Americans did more than the White House. By voluntarily agreeing to months of social distancing, they bought the country time, at substantial cost to their financial and mental well-being. Their sacrifice came with an implicit social contract—that the government would use the valuable time to mobilize an extraordinary, energetic effort to suppress the virus, as did the likes of Germany and Singapore. But the government did not, to the bafflement of health experts. “There are instances in history where humanity has really moved mountains to defeat infectious diseases,” says Caitlin Rivers, an epidemiologist at the Johns Hopkins Center for Health Security. “It’s appalling that we in the U.S. have not summoned that energy around COVID‑19.”
Instead, the U.S. sleepwalked into the worst possible scenario: People suffered all the debilitating effects of a lockdown with few of the benefits. Most states felt compelled to reopen without accruing enough tests or contact tracers. In April and May, the nation was stuck on a terrible plateau, averaging 20,000 to 30,000 new cases every day. In June, the plateau again became an upward slope, soaring to record-breaking heights.
[Read: Ed Yong on living in a patchwork pandemic]
Trump never rallied the country. Despite declaring himself a “wartime president,” he merely presided over a culture war, turning public health into yet another politicized cage match. Abetted by supporters in the conservative media, he framed measures that protect against the virus, from masks to social distancing, as liberal and anti-American. Armed anti-lockdown protesters demonstrated at government buildings while Trump egged them on, urging them to “LIBERATE” Minnesota, Michigan, and Virginia. Several public-health officials left their jobs over harassment and threats.
It is no coincidence that other powerful nations that elected populist leaders—Brazil, Russia, India, and the United Kingdom—also fumbled their response to COVID‑19. “When you have people elected based on undermining trust in the government, what happens when trust is what you need the most?” says Sarah Dalglish of the Johns Hopkins Bloomberg School of Public Health, who studies the political determinants of health.
“Trump is president,” she says. “How could it go well?”
The countries that fared better against COVID‑19 didn’t follow a universal playbook. Many used masks widely; New Zealand didn’t. Many tested extensively; Japan didn’t. Many had science-minded leaders who acted early; Hong Kong didn’t—instead, a grassroots movement compensated for a lax government. Many were small islands; not large and continental Germany. Each nation succeeded because it did enough things right.
[Read: What really doomed America’s coronavirus response]
Meanwhile, the United States underperformed across the board, and its errors compounded. The dearth of tests allowed unconfirmed cases to create still more cases, which flooded the hospitals, which ran out of masks, which are necessary to limit the virus’s spread. Twitter amplified Trump’s misleading messages, which raised fear and anxiety among people, which led them to spend more time scouring for information on Twitter. Even seasoned health experts underestimated these compounded risks. Yes, having Trump at the helm during a pandemic was worrying, but it was tempting to think that national wealth and technological superiority would save America. “We are a rich country, and we think we can stop any infectious disease because of that,” says Michael Osterholm, the director of the Center for Infectious Disease Research and Policy at the University of Minnesota. “But dollar bills alone are no match against a virus.”
Public-health experts talk wearily about the panic-neglect cycle, in which outbreaks trigger waves of attention and funding that quickly dissipate once the diseases recede. This time around, the U.S. is already flirting with neglect, before the panic phase is over. The virus was never beaten in the spring, but many people, including Trump, pretended that it was. Every state reopened to varying degrees, and many subsequently saw record numbers of cases. After Arizona’s cases started climbing sharply at the end of May, Cara Christ, the director of the state’s health-services department, said, “We are not going to be able to stop the spread. And so we can’t stop living as well.” The virus may beg to differ.
At times, Americans have seemed to collectively surrender to COVID‑19. The White House’s coronavirus task force wound down. Trump resumed holding rallies, and called for less testing, so that official numbers would be rosier. The country behaved like a horror-movie character who believes the danger is over, even though the monster is still at large. The long wait for a vaccine will likely culminate in a predictable way: Many Americans will refuse to get it, and among those who want it, the most vulnerable will be last in line.
Still, there is some reason for hope. Many of the people I interviewed tentatively suggested that the upheaval wrought by COVID‑19 might be so large as to permanently change the nation’s disposition. Experience, after all, sharpens the mind. East Asian states that had lived through the SARS and MERS epidemics reacted quickly when threatened by SARS‑CoV‑2, spurred by a cultural memory of what a fast-moving coronavirus can do. But the U.S. had barely been touched by the major epidemics of past decades (with the exception of the H1N1 flu). In 2019, more Americans were concerned about terrorists and cyberattacks than about outbreaks of exotic diseases. Perhaps they will emerge from this pandemic with immunity both cellular and cultural.
There are also a few signs that Americans are learning important lessons. A June survey showed that 60 to 75 percent of Americans were still practicing social distancing. A partisan gap exists, but it has narrowed. “In public-opinion polling in the U.S., high-60s agreement on anything is an amazing accomplishment,” says Beth Redbird, a sociologist at Northwestern University, who led the survey. Polls in May also showed that most Democrats and Republicans supported mask wearing, and felt it should be mandatory in at least some indoor spaces. It is almost unheard-of for a public-health measure to go from zero to majority acceptance in less than half a year. But pandemics are rare situations when “people are desperate for guidelines and rules,” says Zoë McLaren, a health-policy professor at the University of Maryland at Baltimore County. The closest analogy is pregnancy, she says, which is “a time when women’s lives are changing, and they can absorb a ton of information. A pandemic is similar: People are actually paying attention, and learning.”
Redbird’s survey suggests that Americans indeed sought out new sources of information—and that consumers of news from conservative outlets, in particular, expanded their media diet. People of all political bents became more dissatisfied with the Trump administration. As the economy nose-dived, the health-care system ailed, and the government fumbled, belief in American exceptionalism declined. “Times of big social disruption call into question things we thought were normal and standard,” Redbird told me. “If our institutions fail us here, in what ways are they failing elsewhere?” And whom are they failing the most?

Americans were in the mood for systemic change. Then, on May 25, George Floyd, who had survived COVID‑19’s assault on his airway, asphyxiated under the crushing pressure of a police officer’s knee. The excruciating video of his killing circulated through communities that were still reeling from the deaths of Breonna Taylor and Ahmaud Arbery, and disproportionate casualties from COVID‑19. America’s simmering outrage came to a boil and spilled into its streets.
Defiant and largely cloaked in masks, protesters turned out in more than 2,000 cities and towns. Support for Black Lives Matter soared: For the first time since its founding in 2013, the movement had majority approval across racial groups. These protests were not about the pandemic, but individual protesters had been primed by months of shocking governmental missteps. Even people who might once have ignored evidence of police brutality recognized yet another broken institution. They could no longer look away.
It is hard to stare directly at the biggest problems of our age. Pandemics, climate change, the sixth extinction of wildlife, food and water shortages—their scope is planetary, and their stakes are overwhelming. We have no choice, though, but to grapple with them. It is now abundantly clear what happens when global disasters collide with historical negligence.
COVID‑19 is an assault on America’s body, and a referendum on the ideas that animate its culture. Recovery is possible, but it demands radical introspection. America would be wise to help reverse the ruination of the natural world, a process that continues to shunt animal diseases into human bodies. It should strive to prevent sickness instead of profiting from it. It should build a health-care system that prizes resilience over brittle efficiency, and an information system that favors light over heat. It should rebuild its international alliances, its social safety net, and its trust in empiricism. It should address the health inequities that flow from its history. Not least, it should elect leaders with sound judgment, high character, and respect for science, logic, and reason.
The pandemic has been both tragedy and teacher. Its very etymology offers a clue about what is at stake in the greatest challenges of the future, and what is needed to address them. Pandemic. Pan and demos. All people.
This article appears in the September 2020 print edition with the headline “Anatomy of an American Failure.”